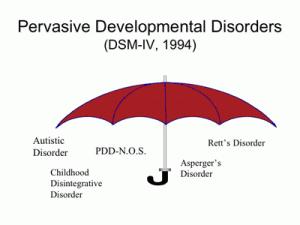
Pervasive Developmental Disorders (PDD)
are a class of conditions to which Autism, Asperger's, Rett Syndrome and others belong. It is not a diagnosis in and of itself.
It is simply a descriptive term. Each of the PDD conditions has specific diagnostic criteria which
must be met in order to satisfy the requirements of the DSM IV.
CUTTING THROUGH THE PSYCHOBABBLE:
DIAGNOSING AUTISM AND PDD-NOS PER THE DSM-IV IN LAYMAN’S
TERMS
This document was born out of confusion experienced by so many
parents about the diagnosis of autism or PDD-NOS. When comparing notes, we discovered that even our physicians did not
agree. One woman told us her psychologist said that a diagnosis of PDD-NOS was reserved for children on the spectrum
who are curable; others have been told that PDD-NOS is not even on the spectrum! We found that many clinicians seem
to take a milder diagnosis and simply label it PDD-NOS.
This document takes the DSM-IV criteria for autism and PDD-NOS
and translates it into English. It also attempts to clarify how a diagnosis of PDD-NOS is made. Please note that
not all symptoms may not be present every day. Look at typically developing children of same age (peers) and use them
as markers. This document is certainly not a diagnostic tool; it was created by and for parents.
To make this easy, (1), (2), (3) are categories, the letters (a),
(b); etc that appear under each category will be referred to as symptoms.
DSM-IV Criteria for Autism
299.00 Autism
A. To be diagnosed with autism, you
must have:
o At least SIX (6) of
the below symptoms from categories (1), (2) and (3).
o You must have TWO (2)
symptoms from (1- Social)
o And ONE (1) each from
(2- Communication) and (3 Behaviors and Interests)
o The other one (or more)
can be from any of the categories.
(1) SOCIAL
Social interaction is impaired, must have TWO from below list of
symptoms:
(a) Problems with nonverbal behaviors such as eye contact,
facial expression, body postures and gestures used in social situations
Examples:
o Eye contact –
different from peers, may only meet eye-gaze of certain people or have total lack of eye contact – or anything in between
o Facial expression –
may seem inappropriate to what the situation warrants, may have blank gaze, may not greet you with a smile, may have same
expression on face most of time – or any combination thereof
o Body Postures –
may hold arms close to sides, may try to avoid certain types of social contact, may appear unapproachable due to posture
o Gestures – may
not respond to a hand held out to shake hands, arms out for hugs etc. May not understand social ‘cues’ we
take for granted
(b) Does not make friends like other children in same age
group.
Examples:
o While peers are learning
to play together, the child is off by themselves
o Children learn to play
by imitation, this child is not imitating the other kids
o Seems to have no interesting
in socializing with peers
o May approach peers,
but not to play…watch and see if the child is approaching in the same way peers approach each other
(c) Does not share objects with others for enjoyment.
Examples:
o Does not bring you
something that interests them to share with you
o Does not point in the
distance (i.e. to an airplane) to share with you something that interests them
o Look at peers and how
they show things they are proud of (ie. Artwork) and see if child does the same thing
(d) Lack of social (Consisting in dealings or
communications with others) and emotional (characterized by emotion) ‘give and take’; Does not respond to social
or emotional cues
Examples:
o Does not seem to seek out or enjoy
the company of others; may be aloof
o Does not smile back when you smile
at him/her (without prompting)
o Does not reply “hello”
to your greeting (without prompting)
o Does not seem especially happy
to see you when you return home after work
o Does not seem to pick up on the
‘vibes’ of others
o Does not become grateful or excited
in anticipation of outing or gift (in the same way a peer would)
o Does not attempt to comfort someone
who is crying
(2) COMMUNICATION
Communication difficulties (Must have at least ONE of the below
symptoms):
(a) Delay in, or total lack of, speech, but does not use
gestures to communicate (Delay = not at same level as peers)
Example:
o Does not point to what
s/he wants
o Does not ‘mime’
his/her needs (ie. Mime ‘eating’ if hungry)
o Does not shake or nod
head for ‘no’ or ‘yes’
o Does not shrug shoulders
to show s/he ‘doesn’t know’
(b) If child can speak, cannot start or hold up their end of a
conversation (appropriately)
(c) May echo phrases, words, songs, parts of movies etc.
(d) Does not engage in imaginative play (as peers)
Examples:
o Will not pretend to
drink from toy teacup
o Will not pretend to
brush doll’s hair
o Will not use items
for make belief (i.e. a stick for a cane or a magic wand)
o Will not make dolls
‘talk’ to each other
o Will not take a toy
airplane and ‘fly’ it around the room while saying ‘zoom’
(3) BEHAVIORS AND INTERESTS
Repetitive behaviors, interests, and activities – child may
get angry if this ‘pattern’ is interrupted. Must have at least ONE of the below symptoms:
(a) Child is so focused on an interest that to remove the interest
will result in a meltdown
(b) Routines or rituals must be followed, they appear to have no
function
Examples:
o Lining up cars is not necessarily
playing ‘garage’; if you attempt to join in, the child will tantrum, walk away, push you aside, etc.
o Family members must always sit
in same seats; failure may result in tantrum
o Must take same route home; one
deviation may cause meltdown
o Must wear red shirt on Tuesday
or risk a tantrum etc
o If you go to the video store, you
must rent “The Brave Little Toaster” every time or risk a tantrum
(c) Repetitive behavior such as hand flapping, rocking, ear flicking,
chewing on clothing, vocal ‘stims’, spinning etc. Establish if this is self-stimulatory by doing a functional
assessment like the Durand Motivational Assessment Scale: http://www.monacoassociates.com/mas/MAS.html
(d) Preoccupied with parts of objects
Examples:
o Spins wheels of toy cars
o Focus on one part of a toy (i.e.
doll’s eyes)
o Cover parts of book so that s/he
can look at one piece
B. Child is either delayed (not same ‘age’ as peers)
or acts differently from peers in ONE of the following (must be noticeable before age three): (1) social interaction, (2)
language as used in social communication, or (3) pretend play.
C. Child does NOT have Rett’s or Childhood Disintegrative
Disorder
299.80 Pervasive Developmental Disorder, Not Otherwise Specified
PDD-NOS is a diagnosis by exclusion. If a child presents
with some symptoms from (1), (2), and/or (3), and their pattern of symptoms is not better described by one of the other PDD
diagnoses (i.e., Autistic Disorder, Asperger’s Disorder, Rett’s Disorder, or Childhood Disintegrative disorder)
then a professional might decide that a diagnoses of PDD-NOS is warranted.
When comparing PDD-NOS to Autism, PDD-NOS is used when a child
has symptoms of autism as above, but not in the configuration needed for an autism diagnosis. Social component is where
the most impairment is seen. Children who fail to meet criteria for autism and don’t have adequate social impairment
typically have a developmental disability, and their symptoms can by accounted for by that.
Looking at above description:
“299.00 Autism - To be diagnosed
with autism, you must have at least 6 of the below symptoms from (1), (2) and (3). You must have two symptoms from (1)
and one each from (2) and (3) – the other two can be any of the other symptoms.”
PDD-NOS is most often diagnosed when children have significant
social impairments, but don’t have the symptoms in area (3). A child with PDD-NOS may have the same (or more,
or less) number of symptoms as a child with autism, but instead of having 2 from #1 and one each from #2, the child might
have 1 symptom from #1 and one from #2, plus two from #3.
A diagnosis of PDD-NOS is not necessarily a less-severe one than
a diagnosis of autism, but can be sometimes.
Severity of any spectrum disorder can be determined by the amount
and severity of symptoms listed above.
It is imperative to obtain a thorough psychological assessment
performed. If you do not understand during any part of the assessment, ask questions. You should feel comfortable
to go home and ‘digest’ the information given to you, form any questions or concerns and contact the diagnosing
clinician to get your answers.
Many thanks go out to R.C. for her help with this project!
A notice to our readers...
This document was put together with input from parents, not physicians.
It is not to be used as a diagnostic tool, nor is it to be considered professional advice.
This document references web sites that may be of interest to the
reader. BBB Autism Support Network makes no presentation or warranty with respect to the accuracy or completeness of
the information contained on any of these web sites, and specifically disclaims any liability for any information contained
on, or omissions from, them. Reference to these web sites herein shall not be construed to be an endorsement of them
or of the information contained thereon, by BBB Autism Support Network.
(c) BBB Autism – July 2002
This document is the intellectual property of BBB Autism
Support Network.
Permission to reproduce and hand out is granted, provided
the document is displayed in its entirety. Other permissions may be requested by email: liz@deaknet.com. The purpose of this copyright is to protect your
right to make free copies of this paper for your friends and colleagues, to prevent publishers from using it for commercial
advantage, and to prevent ill-meaning people from altering the meaning of the document by changing or removing a few paragraphs.
Source Url: http://www.bbbautism.com/diagnostics_psychobabble.htm